
Health Care & Wellness
PDAB Implementation Challenges Slow State Drug Cost Efforts
June 8, 2026 | Mary Kate Barnauskas
April 1, 2026 | Mary Kate Barnauskas

Key Takeaways:
Following a wave of state and federal activity in 2025, the access and practice of fertility care has become a notable issue in state health policy debates. As a result, state lawmakers are increasingly assessing coverage requirements for fertility care, such as in vitro fertilization and fertility preservation, as part of efforts to address affordability and access.
Currently, 25 states and Washington, D.C. require private insurance coverage for fertility care, although mandates vary significantly in terms of who and what they cover. Coverage requirements differ and may include diagnosis of infertility, treatment of underlying causes, assisted reproductive technologies, such as in vitro fertilization (IVF), fertility preservation, and/or fertility drugs. State coverage laws also limit who may qualify for required fertility benefits, with many states establishing age restrictions, marital status, or medical diagnosis requirements. In particular, several states only require coverage for fertility preservation for iatrogenic infertility, which refers to infertility caused by medically necessary treatments, such as chemotherapy or other interventions that may impair reproductive ability.
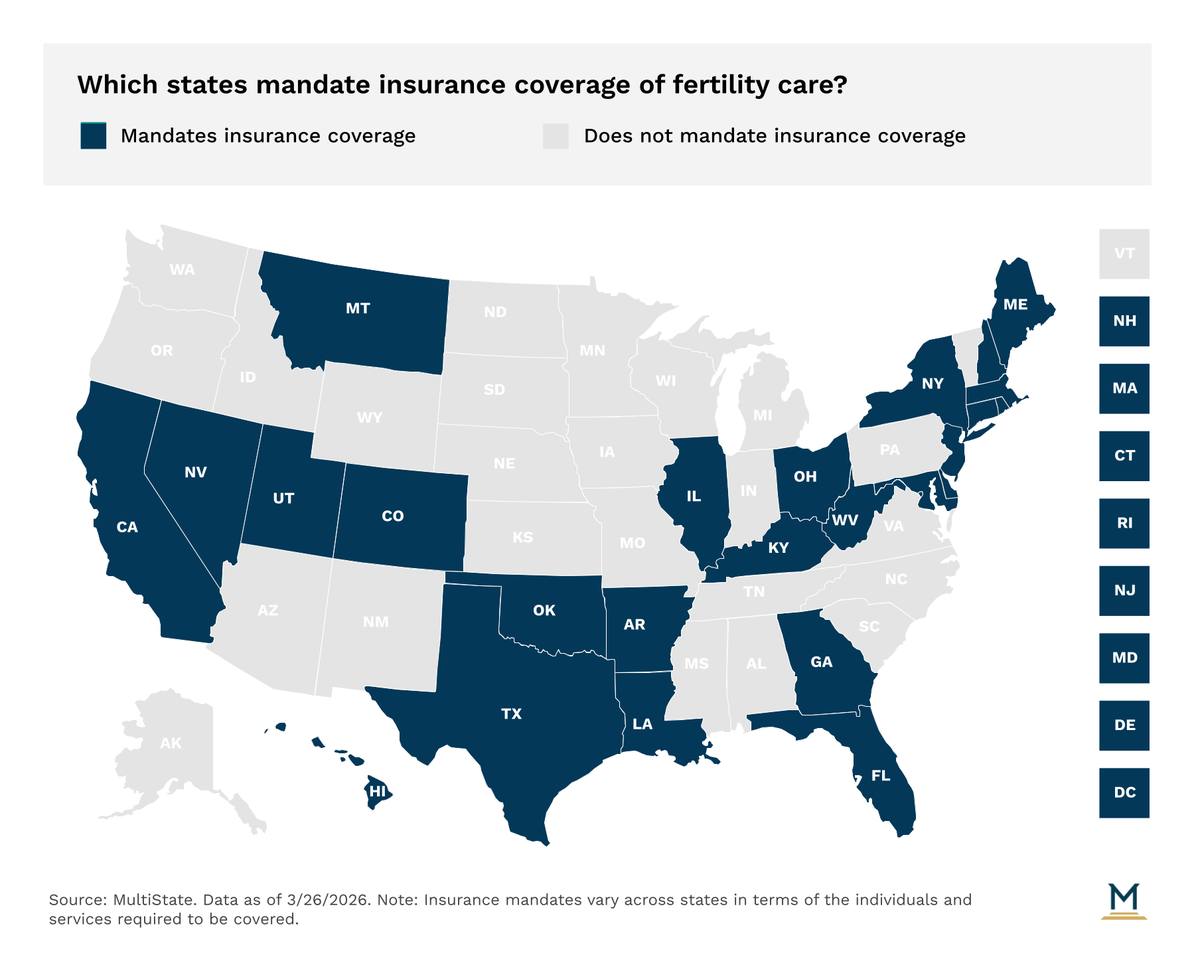
Medicaid coverage for fertility treatment is even more limited than in the commercial market. State Medicaid programs generally do not provide coverage for comprehensive fertility care, including assisted reproductive technologies like IVF. New York, Utah, and Washington, D.C are the only states that offer Medicaid coverage for infertility treatments, but even then the coverage is limited. In New York and Washington, D.C., Medicaid coverage is restricted to three cycles of ovulation-inducing medications, and Utah implemented a state plan amendment in 2024 to provide Medicaid coverage for IVF and genetic testing but only for carriers of certain genetic diseases. Similar to the private market, the most common covered benefit under Medicaid programs is fertility preservation for those with iatrogenic infertility, with 5 states requiring such coverage.
States are following trends from last year with over half introducing or carrying over legislation related to commercial or Medicaid coverage of fertility care this session. Under growing budget pressures, few states are considering Medicaid coverage for fertility care, but there has been sustained activity in 2026 related to coverage mandates in the commercial market. State activity in 2026 suggests a continued focus on targeted, incremental changes as policymakers weigh access, affordability, and benefit design.
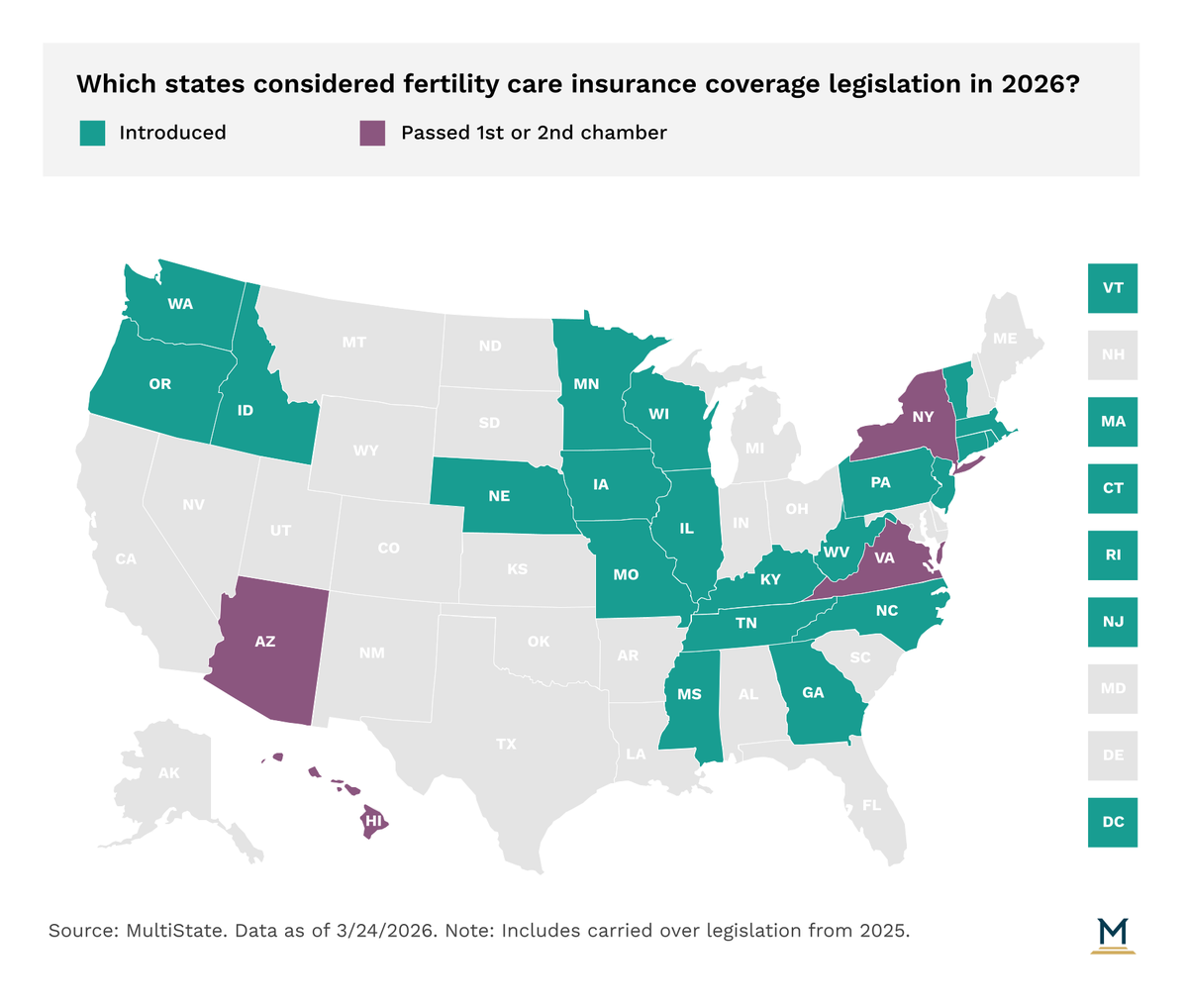
Of note, the Virginia General Assembly enrolled legislation (VA HB 328) that would require the Bureau of Insurance to select a new essential health benefits benchmark plan for the 2028 plan year that includes coverage for the treatment of iatrogenic infertility, fertility treatment and diagnosis, including a maximum of three cycles per lifetime of assisted reproductive technology. The bill was a recommendation from the Commonwealth’s Health Insurance Reform Commission after it reviewed the inclusion of such benefits last year in response to legislation passed in 2024 directing the Commission to do so.
Following existing trends, Arizona and Hawaii are moving legislation to require coverage for iatrogenic infertility. In Arizona, the Senate passed a bill (AZ SB 1347) that would require insurers to provide coverage for standard fertility preservation services for a member within reproductive age, who is diagnosed with cancer, and whose medically necessary treatment is likely to cause iatrogenic infertility. Similarly, in Hawaii the House passed legislation (HI HB 1684) that would require insurance coverage for standard fertility preservation services for individuals undergoing medically necessary treatment that may cause iatrogenic infertility. Both bills have been reported by committees in the opposite chamber, and could see additional movement before the legislatures adjourn. Lawmakers in Idaho considered but ultimately opted not to move a similar measure (ID HB 818) in committee this year, and the New York Senate had previously passed legislation (NY S 4497) in 2025 that carried over.
In Connecticut and Rhode Island, lawmakers have considered a study approach to the issue. In Rhode Island, HR 7951 would create a 17-member special legislative commission to study and make recommendations on women’s reproductive health across the life course, including fertility and infertility, including the adequacy of public and private insurance coverage for reproductive health services, treatment, and conditions. The bill received a committee hearing, but was ultimately held for further study. Meanwhile, in Connecticut, HB 5374 as introduced would have required the Insurance Commissioner to study mandated health insurance coverage for several different healthcare services, including infertility medical treatment or services. However, in the committee process the bill was substituted to mandate insurance coverage for several services, and notably expanded the definition of “infertility” under the state’s current coverage mandate.
Although interest in expanding fertility coverage continues to grow, trends suggest continued variation in coverage across states and markets. With many states wrapping up regular sessions in the spring, additional movement on pending legislation could further influence the coverage landscape. As states continue to evaluate coverage options, lawmakers may look to refine existing mandates and advance narrower expansions of coverage rather than sweeping reforms.
The ever-evolving state health policy landscape will continue to influence how health care organizations make business decisions. MultiState’s team pulls from decades of expertise to help you effectively navigate and engage. MultiState’s team understands the issues, knows the key players and organizations, and we harness that expertise to help our clients effectively navigate and engage on their policy priorities. We offer customized strategic solutions to help you develop and execute a proactive multistate agenda focused on your company’s goals. Learn more about our Health Care Policy Practice.
June 8, 2026 | Mary Kate Barnauskas

May 12, 2026 | Mary Kate Barnauskas

April 1, 2026 | Mary Kate Barnauskas